[SS-072]
Multiple Taşlı Transplante Böbrekli Olguda Retrograd İntrarenal Cerrahi ve Mini Perkütan Nefrolitomi Tekniklerinin Kombine Kullanımı
Mesut Tek, Erdem Akbay, Murat Bozlu, Hasan Erdal DorukGİRİŞ: Son dönem böbrek yetmezliği hastalarının tedavisinde renal transplantasyon uzun sağkalım ve daha iyi yaşam kalitesi sunması nedeniyle diyalizden daha iyi bir tedavi alternatifi haline gelmiştir. Günümüzde renal tarnsplantasyon sayısında görülen artışla birlikte gerek nakile bağlı gerekse nakilden bağımsız ürolojik problemlerin görülme sıklığı da artmaktadır. Donör böbreklerde ürolitiyazis oldukça nadir görülen bir durum olup insidansı %1’in altındadır.
OLGU: 23 yaşında, Aralık 2012’de kliniğimizde canlı donörden renal transplantasyon yapılan hasta nefroloji takipleri sırasında transplante böbrekte taş tespit edilmesi üzerine kliniğimize konsülte edildi. Hastanın polikliniğe başvurusu sırasında kasık bölgesinde ağrı ve idrar miktarında azalma şikayetleri bulunmaktaydı. Ultrasonografide renal pelvis çapı 18 mm, pelvisde yaklaşık 11x10 mm ve böbrek alt polünde 2 adet yaklaşık 8x8 mm’lik taşa ait ekojenite izlendi. Pelvik tomografisinde(Resim 1) pelvisde 11 mm ve alt polde 2 adet 8 mm’lik taş izlendi. Hastanın kreatin değerinin 1,1 mg/dl olduğu ve idrar kültüründe üremenin olmadığı gözlendi. Hastaya retrograd intrarenal cerrahi planlandı.
YÖNTEM: Genel anestezi altında litotomi pozisyonunda neoüreter lümeninden dual fleks guide wire yerleştirildi. Floroskopi altında guide wire üzerinden flexible üreteroskop (Wolf Cobra; Richard Wolf, Knittlingen, Germany) ile üreterde ilerlenerek renal pelvisteki taş vizüalize edildi(Resim 2). Taş 200 μm holmium: yttrium-aluminum-garnet lazer fiberi ile 0.8-1.2 J enerji ve 5-10 Hz frekansta toz etme yöntemi ile fragmante edildi. Alt kaliks taşlarına üreteroskopun fleksiyon açısının yetersiz olması nedeniyle ulaşılamadı ve mini-PNL uygulanmasına karar verilerek guide wire üzerinden 5 F üreter kateteri yerleştirildi. Hasta supin pozisyonda iken floroskopi altında retrograd kontrast verilmek suretiyle toplayıcı sistemler vizualize edildi ve 18 G giriş iğnesi ile taşların yer aldığı alt kalikse girildi. Giriş iğnesinden 0,035 mm çapında hidrofilik guidewire gönderilerek floroskopi altında guide üzerinden “one-step bougie” tekniği ile metal dilatatör ile dilatasyon yapıldı. Dilatatör üzerinden 15/16-Ch çalışma kanalı olan(Karl Storz, Tuttlingen, Germany) kılıf alt kaliks içerisine yerleştirilerek 6.7 Ch çalışma kanalı olan 12Ch Karl Storz nefroskop ile girildi. Alt poldeki taşlar forseps yardımıyla dışarı alındı(Resim 3). Daha sonra floroskopi eşliğinde antegrat double J stent yerleştirildi(Resim 4) ve operasyon sonlandırıldı.
SONUÇ: Bu vaka renal transplantasyonlu böbrek taşlarında, gereft böbrekte taşsızlık elde etmek için, RIRC ve mini PNL tekniklerinin tek başına ya da kombine olarak güvenli yöntemler olarak kullanılabileceğini göstermektedir.
Treatment of Multiple Kidney Stone in a Kidney-Transplanted Patient with the Combination of Retrograd Inrarenal Surgery and Mini-Percutaneous Nephrolithotomy
Mesut Tek, Erdem Akbay, Murat Bozlu, Hasan Erdal DorukINTRODUCTION: Kidney transplantation is the treatment choice for patients with end-stage renal disease, because it offers prolonged survival and better quality of life.Nephrolithiasis in a transplanted kidney is an uncommon complication, with an incidence reported less than 1%.
CASE: A 23-year-old girl received a kidney transplant from a living donor in December 2012 admitted to nephrology represented with groin pain and reduction of urine.Ultrasound revealed hydronephrosis (pelvic diameter 18 mm) and multiple stones in the pelvis and lower pole of the transplated kidney.Three stones; 11 mm in renal pelvis and two stones (8 mm) in the lower pole were seen in Pelvic CT scan(Figure 1).Serum creatinine was 1.1 mg/dL and ürine culture was negative. Retrograde intrarenal surgery was planned.
METHOD: Under general anesthesia hydrophilic guide wire was inserted into the pelvicalyceal system through the neouretheral orifice in the lithotomy position. Flexible ureteroscope(Wolf Cobra; Richard Wolf, Knittlingen, Germany) passed through the guide wire into the collecting system under fluoroscopic imaging. The stone was visualized and fragmented with dusting technique using 200 μm holmium:yttrium-aluminum-garnet laser fiber with the settings of 0.8-1.2 J and 5-10 Hz. We failed to access the lower pole stones due to the inadequate flexion angle of the ureteroscope. We decided to perform mini-PNL for the lower pole stones and placed a 5F uretheral catheter through the guide wire. In the supine position lower pole puncture was performed with the 18 gauge access needle and the hydrophilic guide wire with floppy tip was inserted into the pelvicalyceal system. Dilatation was performed by a single metal dilator using the one-step bougie technique.Via this dilator,15/16-Ch operating sheath(Karl Storz, Tuttlingen, Germany) was placed in the renal pelvicalyceal system.Dilation and advancement of the operating sheath was accomplished under floroscopy. Mini-nephroscope(instrument sheath diameter 12 Ch with 6.7 Ch working channel; Karl Storz) was introduced through the operating sheath.The stones were visualized and removed with graspers(Figure3). A single J was placed by antegrad technique under floroscopy control(Figure 4).
CONCLUSION: Our case shows that RIRC and the mini PNL technique can be safely used alone or in combination in transplanted kidney stones to obtain stone free graft.
Resim 1. Transplante böbrek pelvisinde yer alan taşın Bilgisayarlı Tomografideki görüntüsü
Figure 1. CT scan image of the stone in the transplanted kidney

)
Resim 2. Renal pelvisteki taşın fleksible üreteroskopideki görüntüsü
Figure 2. Flexible ureteroscopic image of the pelvic stone.

)
Resim 3. Mini PNL yöntemi ile alt polden çıkarılan taşlar
Figure 3. Images of the stones extracted with mini-PNL from lower pole

)
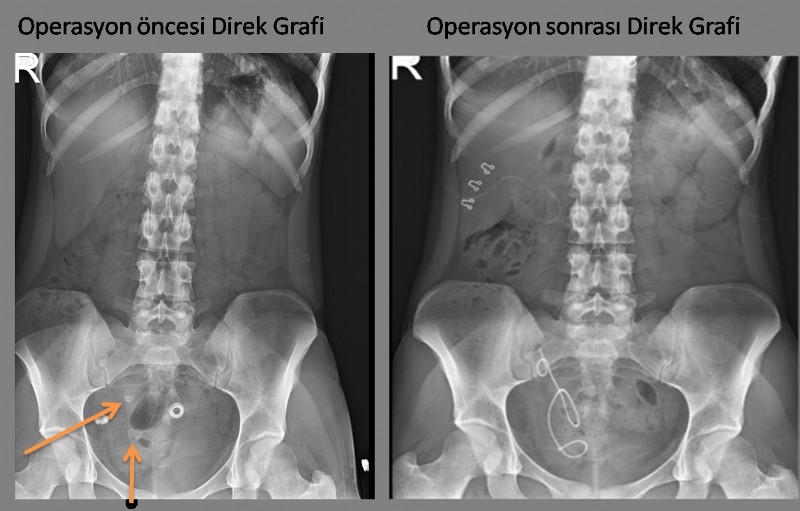
Resim 4. Olgunun preoperatif ve postoperatif direk grafi görüntüleri
Figure 4. Images of preoperative and postoperative direct scans of the case.
)