[SS-211]
Oturum adı: ORAL SESSION 12 | Oturum salonu: SALON 1 | Oturum tarihi: 18 Ekim 2014 | Oturum saati: 09:00 - 11:25Üreteroskopide mukozal hasarı etkileyen faktörler
Tolga Karakan1, Ahmet Metin Hasçiçek1, Arif Demirbaş1, Berkan Reşorlu1, Mehmet Ali Karagöz1, Erim Ersoy1, Muzaffer Eroğlu22Hacettepe Üniversitesi Tıp Fakültesi, Üroloji Ana Bilim Dalı, Ankara
Amaç: Üreter taşı tedavisi sırasında intraoperatif mukozal yaralanmayı etkileyen faktörlerin araştırılması.
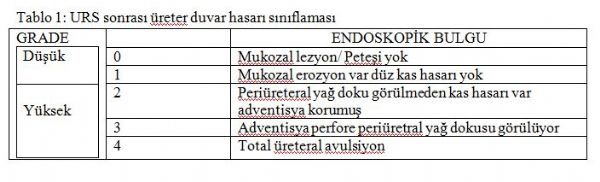
Materyal ve metodlar: Mart 2014 ile Temmuz 2014 tarihleri arasında üreter taşı nedeniyle URS yapılan 102 hastanın verileri değerlendirilmiştir. Tanısal amaçla URS yapılan hastalar çalışmaya dahil edilmemiştir. URS sırasında meydana gelen mukozal yaralanmalar ameliyat sonunda endoskopik olarak değerlendirilmiş olup, Traxer ve ark. tarafından yapılan sınıflamaya göre low grade (grade 0 ve 1) ve high grade (grade 2, 3 ve 4) yaralanmalar olarak iki gruba ayrılmıştır (Tablo 1). Bu iki grup; hasta ve taşa ait karakteristikler, kullanılan litotripsi yöntemi, üreteral dilatasyon yöntemi, preoperative stent varlığı, ameliyat başarısı ve postoperative double-j stent gereksinimi açısından birbiri ile karşılaştırılmıştır.
BULGULAR: Ameliyat sonunda toplam 81 hastada (79.4%) üreteral yaralanma tespit edilmiştir. Endoskopik olarak lezyonlar sınıflandığında; %20.6 grade 0, %44.1 grade 1, %31.4 grade 2 ve %3.9 oranında grade 3 yaralanma tespit edilmiş olup, bizim serimizde grade 4 yaralanmaya rastlanmamıştır. Düşük ve yüksek gradeli mukozal yaralanması olan hasta grupları arasında; yaş, cinsiyet, komorbidite varlığı, taş lokalizasyonu, taş tarafı, ameliyat öncesi ESWL uygulanması, preoperative DJ stent varlığı, litotripsi yöntemi, hidronefroz derecesi ve üreteral dilatasyon yöntemi açısından fark saptanmazken (herbir değer için p>0.05); taş boyutu (12.2 mm vs 14.6 mm), tedavi edilmiş peoperatif enfeksiyon varlığı (%3 vs %16), ameliyat süresi (27.5 dk vs 38.7 dk) ve cerrahi başarı oranı (%90 vs %76) açısından istatistiksel anlamlı fark saptanmıştır (herbir değer için p<0.05).
Tartışma: Mukozal yaralanma evreleme sistemi üreteroskopi sırasındaki lezyonların standardize edilmesi açısından faydalı olabilir. Taş boyutunun artması, ameliyat süresinin uzaması ve preoperatif olarak tedavi edilmiş olsa da enfeksiyon olması ciddi mukozal yaralanma açısından risk faktörü oluşturmaktadır.
Factors affecting mucosal damage during ureteroscopy
Tolga Karakan1, Ahmet Metin Hasçiçek1, Arif Demirbaş1, Berkan Reşorlu1, Mehmet Ali Karagöz1, Erim Ersoy1, Muzaffer Eroğlu22Department of Urology, Hacettepe University Faculty of Medicine, Ankara, Turkey
OBJECTIVE: To evaluate the predictive factors for intra-operative mucosal injury of rigid ureteroscopy (URS) in the treatment of ureteral calculi.
MATERIAL-METHODS: We reviewed the consecutive 102 patients’ data who underwent URS due to the uretheric stone disease between march and July 2014. The only exclusion criteria was diagnostic procedures. The mucosal injuries were evaluated endoscopically after the URS procedure and the injuries divided into two groups as low grade( grade 0 and 1) and high grade (grade 2,3,4) by Traxer et al. classification (Table 1). These two groups; Characteristics of patients and stone, lithotripsy technique, method of ureteral dilatation, preoperative stent presence, operative success and postoperative requirements for a double-J stent was compared with each other.
RESULTS: At the end of surgery ureteral injuries were identified in 81 patients (79.4%). When the lesions classified with endoscopy; 20.6% grade 0, 44.1% grade 1, 31.4% grade 2 and 3.9% grade 3 injury has been identified, no grade 4 injury was observed in our series. Although comparison of low-and high-grade groups of patients with mucosal injury; age, sex, comorbidity, stone location, stone side, preoperative implementation of SWL, preoperative presence of DJ stents, lithotripsy method, the degree of hydronephrosis and ureteral dilatation was no difference between the groups (For each value p>0.05); stone size (12.2 mm vs 14.6 mm), the presence of preoperative treated infection (3% vs 16%), operative time (27.5 min vs 38.7 min) and the surgical success rate (90% vs 76%), statistically significant differences were found (each value of p <0.05).
CONCLUSION: The mucosal injury grading system may be used for standardized reporting of ureteral lesions after ureteroscopy. The increase in stone size, longer duration of surgery and preoperative treated infection constitutes a risk factor for severe mucosal injury.
Tablo 1
Table 1
)