[SS-175]
Oturum adı: ORAL SESSION 9 | Oturum salonu: SALON 2 | Oturum tarihi: 17 Ekim 2014 | Oturum saati: 16:50 - 18:00Seminal Vezikül Kistleri: Tanı ve Tedavi Seçenekleri
Osman Köse, Şükrü Kumsar, Fikret Halis, Hüseyin Aydemir, Adil Emrah Sonbahar, Hacı İbrahim Çimen, Hacı Can Direk, Hasan Salih Sağlam, Ahmet Gökçe, Öztuğ AdsanAMAÇ: Seminal vezikül kistleri 0.005% oranında oldukça nadir karşılaşılan, konjenital veya edinsel olabilen anomalilerdir. Her ne kadar çoğunlukla asemptomatik olsalar da, bu kistler değişik derecelerde farklı semptomlarla kendilerini gösterebilirler. Cerrahi müdahale, transrektal aspirasyon, transüretral unroofing, cerrahi eksizyonu içermekle beraber, seminal vezikül kistlerine cerrahi müdahale yöntemi ile ilgili fikir birliği oluşmamıştır. Bu çalışmada seminal vezikül kistleri ile ilgili tecrübelerimizi sunmayı amaçladık.
YÖNTEM-GEREÇLER: 2011-2013 yılları arasında seminal vezikül kisti saptanan 4 hastanın kayıtları retrospektif olarak değerlendirildi. Hastaların şikayetleri, fertilite durumları, fizik muayene bulguları diagnostik testler, saptanan bulgular, cerrahi müdahaleler, takip süresi, komplikasyonlar, rekürrens, kist duvarının histolojik muayenesi değerlendirildi (Tablo 1).
BULGULAR: Yaşları 21-63 arasında değişen (Ortalama: 37.7) 4 hastada seminal vezikül kisti saptandı (Tablo 1). Üç hasta fertil ve 1 hasta infertildi. Hastaların kliniğe başvuru şikayetleri dev kisti olan bir hastada alt karın ağrısı, iki hastada perineal ağrı, irritatif alt üriner sistem semptomları olarak gözlendi. Dördüncü hasta asemptomatikti. Üç hastada ipsilateral renal agenezi vardı. İki hastaya transüretral rezeksiyon, uygulandı. Kistin transrektal veya transperineal drenajı yüksek enfeksiyon ve rekürrens riski nedeniyle tercih edilmedi.Kist çapı 12 santimetreden büyük dev kisti olan bir hastaya açık rezeksiyon uygulandı (Resim1). Renal agenezisi olan azospermik hastanın postoperatif altıncı ayda hafif alt üriner sistem semptomları dışında tamamen düzeldiği gözlendi ve spermiogram analizinde sperm saptandı. Asemptomatik bir hasta müdahale edilmeden takip edildi. Örneklerin histopatolojik muayenesi seminal vezikül kistiyle uyumlu olduğu rapor edildi. Ortalama takip süresi 8 ay olarak saptandı. Takiplerinde komplikasyon veya rekürrens gözlenmedi.
SONUÇLAR: Dev seminal vezikül kistleri için açık cerrahi yaklaşım kesin tedavi yöntemi olarak kabul edilebilir. Bununla birlikte küçük asemptomatik seminal vezikül kistleri müdahale edilmeden takip edilebilse de, mesaneye protrude semptomatik kistlere transüretral yolla tedavi edilebilir.
Seminal Vesicle Cysts: Diagnosis and Treatment Options
Osman Köse, Şükrü Kumsar, Fikret Halis, Hüseyin Aydemir, Adil Emrah Sonbahar, Hacı İbrahim Çimen, Hacı Can Direk, Hasan Salih Sağlam, Ahmet Gökçe, Öztuğ AdsanINTRODUCTION: Seminal vesicle cyst is an exceedingly rare acquired or congenital pathology, manifesting in less than 0.005% of the population. Although mostly asymptomatic, these cysts can present with varying degrees of different symptoms. Although surgical management consists of transrectal aspiration, transurethral unroofing, or open surgical excision, no consensus on management of seminal vesicle cyst could be reached. We aimed to report our experience on the management of seminal vesicle cyst.
MATERIAL-METHODS: A retrospective chart review was conducted on four patients diagnosed with seminal vesicle cyst between 2011 and 2013. Patients’ complaints, fertility, physical signs, diagnostic tests and the obtained findings, surgical intervention, duration of follow–up period, complications, recurrence and histologic examination of the cysts wall were evaluated in patients included.
RESULTS: Four male patients, aged 21–63 years (mean: 37.7 years) with seminal vesicle cysts were identified. Three patients were fertile and one patient was infertile. The patients’ complaints included lower abdominal pain in one patient with giant seminal vesicle cyst and perineal pain, irritative lower urinary tract symptoms in two patient. Fourth patient was asymptomatic. Three patients have ipsilateral renal agenesia. Two patients were operated with transurethral resection. The transrectal or transperineal drainage of the cyst is not preferred due to high risk of infection and high frequency of recurrence after drainage. Seminal vesicle cyst larger than 12 cm are evaluated as giant cysts and operated with open resection (Figure 1). The patient with azoospermia and renal agenesis recovered completely at postoperative month 6 except symptoms of mild lower urinary tract symptoms and his spermiogram analysis was positive for sperms. One asymptomatic patient followed without intervention. Histopathologic examination of the samples were reported to be compatible with seminal vesicle cyst. The mean follow–up period was 8 months (range: 6–12 months). Neither complications nor recurrences were observed.
CONCLUSIONS: The open surgical approach might be considered the definitive form of treatment for giant cysts. Athough small asymptomatic seminal vesical cyst can be followed without intervention, the symptomatic cyst protruding to bladder can be managed by transurethral route.
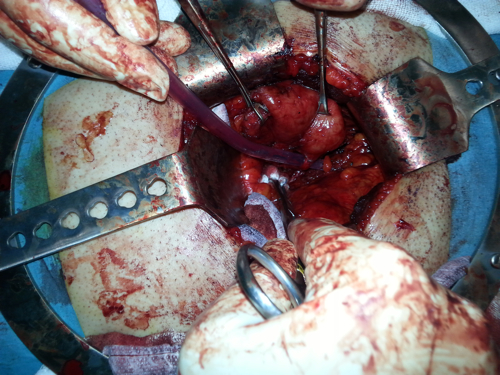
Resim 1
Figure 1
)
Dev kistli hastanın açık cerrahi görüntüsü
Surgical view of the patient with giant cyst
Table 1
| Olgu 1 | Olgu 2 | Olgu 3 | Olgu 4 | |
| Yaş | 21 | 39 | 28 | 63 |
| Kist Boyutu (cm) | 4x5 | 20x25 | 4x5 | 6x5 |
| Baskın Şikayet | Perineal ağrı, dizüri, pollakiüri | Sol alt kuadradranda künt ağrı | Perineal ağrı, dizüri, pollakiüri | Yok |
| Renal Agenezi | (-) | (+) | (+) | (+) |
| Cerrahi | TUR | Açık rezeksiyon | TUR | (-) |
| Operasyon Süresi (dk) | 34 | 58 | 30 | (-) |
| Komplikasyon | (-) | (-) | (-) | (-) |
| Hastane yatış süresi (gün) | 2 | 3 | 2 | (-) |
Hasta Özellikleri
Table 1
| Case 1 | Case 2 | Case 3 | Case 4 | |
| Age | 21 | 39 | 28 | 63 |
| Cyst Size (cm) | 4x5 | 20X25 | 4X5 | 6x5 |
| Dominant Symptom | Perineal pain, dysuria,pollakuria | Left quadrant dull pain | Perineal pain, dysuria,pollakuria | None |
| Renal Agenesis | (-) | (+) | (+) | (+) |
| Surgery | TUR | Open resection | TUR | (-) |
| Operation Time (min) | 34 | 58 | 30 | (-) |
| Complication | (-) | (-) | (-) | (-) |
| Hospitalisation Period (day) | 2 | 3 | 2 | (-) |
Patient Characteristics