[P-290]
Oturum adı: POSTER SESSION 5 | Oturum salonu: POSTER AREA | Oturum tarihi: 18 Ekim 2014 | Oturum saati: 14:00 - 19:00Üretral stenozun eşlik ettiği Johanson Blizzard Sendromu: Olgu sunumu
Esra Meltem Kayahan Ulu1, Dilek Polat2, Didem Yeşilırmak3, Özlem Sezer4, Ünal Bıçakçı5, Beytullah Yağız5, Abdullah Açıkgöz6, Muhammed Bahattin Ulu72Samsun Medikalpark Hastanesi, Çocuk Cerahisi Bölümü
3Samsun Medikalpark Hastanesi, Çocuk Hastalıkları Bölümü
4Samsun Eğitim ve Araştırma Hastanesi, Tıbbi Genetik Bölümü
5Ondokuzmayıs Üniversitesi Tıp Fakültesi, Çocuk Cerrahisi Bölümü
6Samsun Medikalpark Hastanesi, Üroloji Bölümü
7Gazi Devlet Hastanesi, Üroloji Bölümü
GİRİŞ: Johanson Blizzard Sendromu (JBS) nadir görülen otozomal resesif bir hastalıktır. Hastalığın 15q15-21 kromozomunda lokalize olan UBR1 geninin mutasyonundan kaynaklandığı gösterilmiştir. Hastalığın tipik klinik özellikleri ekzokrin pankreas yetersizliği, burun kanadı hipoplazisi, konjenital saçlı deri defektleri, sensorinöral duyma kaybı, büyüme geriliği, psikomotor gerilik, hipotiroidizm, imperfore anüs, ve ürogenital anomalilerdir. JBS tanısı konulan yenidoğanda posterior üretral valv olmaksızın üretral stenozun neden olduğu ürogenital sistem komplikasyonlarının klinik ve radyolojik bulguları sunuldu.
MATERYAL-METOD: Sezaryen ile 2400 gram doğan ve antenatal takiplerinde batında kistik kitle nedeni ile takip edilen erkek olgu kliniğimize başvurdu.
BULGULAR: Fizik muayenede batında distansiyon, anal atrezi, sağda inmemiş testis ve skrotumda hipoplazi saptandı. Penil muayenesinde üretral meatus normal lokalizasyonda idi ancak devamlılığı izlenmedi ve penis şaftında prepisyumun üzerinde ikinci bir meatus mevcuttu. Ala nazilerde hipoplazi, gaga burun, seyrek saçlar ve skalp aplazi kutis konjenita mevcuttu. Olguya yapılan abdominal USG tetkikinde her iki böbrekte kistik hidronefroz mevcuttu Bilateral üreterlerde belirgin dilatasyon mevcuttu. Pelviste rektum lokalizasyonunda 25x18 mm boyutlarında atretik anal poşa ait olduğu düşünülen kistik yapı izlendi. Olguya kolostomi ve sistofiks açıldı. Sistofiks yoluyla yapılan sistografide sağda grade IV VUR tespit edildi, solda VUR saptanmadı. Tüm abdomen MRG tetkikinde USG tetkikinde saptanan bulgulara ek olarak her iki üreter distal segmentinin normal lokalizasyonda olduğu saptandı ancak üreter alt uçları vizualize edilemediğinden belirgin stenotik olduğu düşünüldü. Bunun üzerine olguya genel anestezi altında penis şaftının ortasındaki üretral yoldan girildi, iğne ucu kadar dar olduğundan mesaneye ulaşılamadı. Sistofiks yolundan sistoskopla yapılan mesane incelemesinde ise sol üretral orifiste stadyum görüntüsü mevcuttu. Üretraya geçiş izlenemedi. Olguya üretral stenoz tanısı konuldu ve vezikostomi açıldı.
SONUÇ: JBS’li olgularda mikropenis, hipospadias, kliteromegali, kriptorşidizm, çift vajen, septat vajen, üretrovajinal fistül, VUR, hidronefroz, kaliektazi gibi genitoüriner anomaliler tanımlanmıştır. %39’ unda ise imperfore anüs görülür. JBS, urogenital sistem anomalileri, pankreasın ekzokrin fonksiyon yetersizliği, burun kanatlarının yokluğu ve imperfore anüs bulguları olan yenidoğan olgularında ayırıcı tanıda akılda tutulması gereken nadir sendromlardandır.
Johannson Blizzard Sendrome with urethral stenosis: Case report
Esra Meltem Kayahan Ulu1, Dilek Polat2, Didem Yeşilırmak3, Özlem Sezer4, Ünal Bıçakçı5, Beytullah Yağız5, Abdullah Açıkgöz6, Muhammed Bahattin Ulu72Samsun Medicalpark Hospital, Department of Pediatric Surgery
3Samsun Medicalpark Hospital, Department of Pediatry
4Samsun Hospital, Department of Medical Genetic
5Ondokuzmayıs Üniversitesi Faculty of Medicine, Department of Pediatric Surgery
6Samsun Medikalpark Hastanesi, Department of Urology
7Gazi State Hospital, Department of Urology
AIM: Johanson Blizzard Sendrome (JBS) is a rare autosomal recessive disorder. The patients with the disease had UBR1 gene mutation localised on 15q15-21 chromosome. The typical features of the disease are exocrin pancreas insufficiecy,hypoplasia of alae nasi, congenital scalp dermal defects, sensorineural hearing loss, growth retardation, psychomotor retardation, hypothyroidism, imperforate anüs, and urogenital anomalies. We report the clinical and radiological findings of the patient diagnosed as JBS and had urethral stenosis without posterior urethral valve.
MATERIALS-METHODS: 2400 grams weighted baby, borned by caesarean section was followed due to abdominal cystic mass in antenatal follow-up applied to our hospital.
RESULTS: The abdominal distension, anal atresia, the right undescended testis, hypoplasia of scrotum were detected on physical examination. Penile examination showed urethral meatus in normal position but not continued süperiorly. In addition second meatus was detected on prepicium of penile shaft. Hypoplasia of alae nasi, beaked nose, sparse hairs, scalp aplasia cutis congenita were detected. Abdominal ultrasonography showed cystic hydronephrosis of both kidneys, There were bilateral ureteral dilatation. The 25x18 mm sized cystic lesion was detected in the pelvis, thought to be belonged to atretic anal pouch. The colostomy ad cystofix was opened. There was grade IV VUR on the right in cystography made through cystofix. No VUR was detected on the left. The abdominal MRI showed that the distal ureters were on normal localisations but the ureteral orifices were not demonstrated. We thought that both ureteral orifices were severely stenotic. Under general anesthesia, by cathetarising the penile shaft, we attempted to image bladder. Due to severe stenosis the imaging was not possible. The imaging of the bladder through cystofix showed stadium appearance of the left ureteral orifice. The passage of urethra was not possible. The diagnosis was urethral stenosis and vezicostomy was opened.
CONCLUSION: The micropenis, hypospadias, cliteromegaly, cryptorchidism, double vagina, septate vagina, urteherovaginal fistula, VUR, hydronephrosis, caliectasis were defined in the patients with JBS. The imperforate anus was seen in 39% of the patients. In patients with urogenital system anomalies, exocrin function deficiency of pancreas, deficiency of ala nasi, and imperforate anus JBS must be included in differential diagnosis.
Figür 1
Figure 1
)
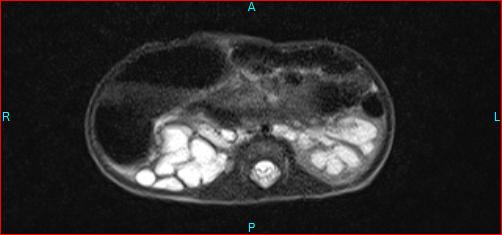
Aksiyel T2 ağırlıklı görüntülerde her iki böbrekte belirgin hidroüreteronefroz izlendi. Sol böbrek parankimi belirgin ince idi.
Axial T2 weighted images showed bilateral severe hydronephrosis on both kidneys. The parenchyma of right kidney was very thin.
Figür 2
Figure 2
)
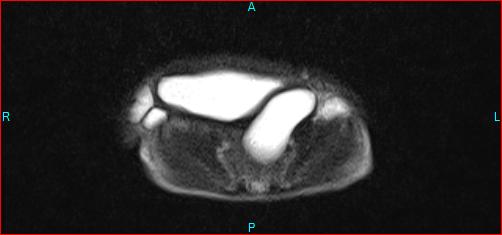
Aksiyel T2 ağırlıklı görüntüde pelviste atretik anal poş izleniyor.
On axial T2 weighted images there was atretic anal pouch in the pelvis.
Figür 3
Figure 3
)
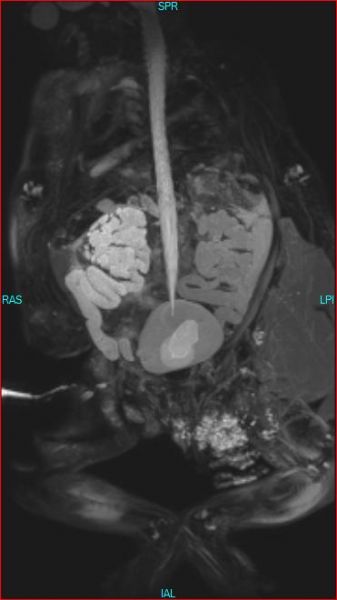
3 boyutlu T2 ağırlıklı rekonstrüksiyon görüntülerde bilateral hidroüreteronefroz ve normal lokalizasyonda üreter alt uçları izleniyor.
On 3D T2 weighted images bilateral hydronephrosis and normal localisations of distal ureters were seen.
Figür 4
Figure 4

)
Sistofiks yolu ile yapılan sistouretrografi tetkikinde sağda grade IV VUR saptanırken sağda VUR saptanmadı.
The cystographic examination by cystofix showed grade IV VUR on the right kidney, but did not show VUR on the left kidney.