[P-286]
Oturum adı: POSTER SESSION 5 | Oturum salonu: POSTER AREA | Oturum tarihi: 18 Ekim 2014 | Oturum saati: 14:00 - 19:00Atipik testiküler torsiyon: Manuel detorsiyon sırasında dikkatli olmalıyız
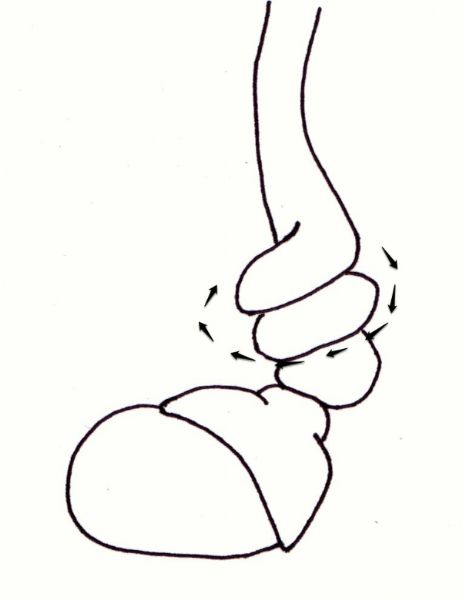
Mustafa Güneş, Mehmet Umul, Muammer AltokGİRİŞ: Testiküler torsiyon yaygın önemli bir ürolojik acildir. Testisler genellikle medial (iç) yönde çeşitli derecelerde rotasyona uğrar (Resim 1). Manuel detorsiyon ameliyathaneye alınmada gecikme olan hastalarda testis canlılığının korunmasına izin veren kritik bir manevradır. Manuel detorsiyon torsiyon yönünün tersine, yani genellikle dışa doğru gerçekleştirilir. Testis torsiyonu nadiren lateral doğrultuda oluşur. Bu durum manuel detorsiyon geçiren hastalar için önemlidir.
OLGU: 14 yaşında çocuk 24 saattir süren sol skrotal ödem ve eritem şikayeti ile kliniğimize sevk edildi. Genital muayenesinde sol hemiskrotumda yüksek transvers posizyonda hassas sol testis ve belirsiz kramasterik refleks görüldü. Sağ testis boyutu ve konumu normaldi. Doppler ultrasonik değerlendirme sol testis arter kan akımının olmadığını gösterdi. Ameliyat öncesi 360 derece dışa manuel detorsiyon denendi, fakat hastada rahatlama görülmedi. Skrotal rafe insizyonu ile eksplorasyon gerçekleştirdik ve 900 derece lateral torsiyone sol testiste hemoraji ve nekrozis gözlemledik (Resim 2). Daha sonra sol orşiektomi ve sağ orşiopeksi uyguladık.
SONUÇ: Manuel detorsiyon için lateral (dışa) rotasyon tavsiye edilmesine rağmen, direnç gelişmesi veya ağrının sürmesi lateral (dışa) dönmenin belirtileri olabilir. Ayrıca, inkomplet torsiyon (<360 °) olduğunda direnç oluşmayabilir. Sonuç olarak, manuel detorsiyon optimum dönemde (6-12h) tıbbi bakım arayan uygun olgularda önemli bir tedavi opsiyonudur. Ancak, hastalarda atipik torsiyon akılda tutulmalıdır.
Atypical testicular torsion: we must be cautious in the course of manual detorsion
Mustafa Güneş, Mehmet Umul, Muammer AltokINTRODUCTION: Testicular torsion is a common important urological emergency. Testicles usually undergo various degrees of rotation in an medial (inward) direction (Figure 1). Manual detorsion is a critical maneuver allowing the preservation of testicular viability in patients with a delay to get into the operation room. Manual detorsion, torsion in the opposite direction, that is usually carried outwardly. Testis torsion rarely occurs in lateral direction. It is important for patients undergoing manual detorsion.
CASE: A 14-year-old boy was referred to our clinic with left scrotal swelling and erythematous for 24 hours. Genital examination revealed a tenderness of left testicle that was high riding with a transverse lie and an ambiguous cremasteric reflex. The right testis was normal in size and position. Doppler ultrasonic evaluation indicated complete absence of left testicular arterial flow. Preoperative manual detorsion 360 degrees outward tried, but did not relieve the patient was seen. We performed scrotal raphe incision and exploration and observed a 900° lateral outward torsion of the left testis with hemorrhage and necrosis (Figure 2). Afterwards, we performed left orchiectomy and right orchiopexy.
CONCLUSION: Although lateral (outward) rotation is recommended for manual derotation, the development of resistance or persistant pain may be signs of the lateral (outward) rotation. Furthermore, a resistance may not ocur in the presence of incomplete (<360°) torsion. In conclusion, manual detorsion is a considerable treatment option in suitable cases seeking for medical care in the optimal period (6-12h). However, atypical torsion cases should be kept in mind.
Resim 1. Testisler genellikle spermatik kordun anteromedial rotasyonu ile içe doğru (medial) yönünde burulur (sol testis şematik görünümü)
Figure 1. Testes usually twist in an inward (medial) direction with anteromedial rotation of the spermatic cord (schematic view of left testis)
)
Resim 2. 24 saat boyunca lateral (dışarı doğru) dönme (900°) sonucu sol nekrotik testis
Figure 2. Left necrotic testis in consequence of lateral (outward) rotation for 24h (900°)

)