[P-100]
Oturum adı: POSTER SESSION 2 | Oturum salonu: POSTER AREA | Oturum tarihi: 17 Ekim 2014 | Oturum saati: 08:00 - 13:00Böbrek taşına bağlı spontan renal pelvis rüptürü
Arif Özkan, Nusret Can Çilesiz, Fatih Yanaral, Buğra Çetin, Memduh Aydın, Barış NuhoğluGiriş: Medikal destek tedavisi üreteropelvik bileşke (UPB) taşlarının tedavilerinden biridir. Bu taşlar; üriner sistem enfeksiyonuna, hidronefroza veya renal yetmezliğe sebep olabilir. Komplike olmuş taş olgularında cerrahi tedavi gerekebilir. UPB'nin spontan perforasyonunun tanı ve tedavisi zordur ve ek problemleri beraberinde getirir. Bu çalışmada taşa bağlı spontan renal pelvis rüptürü (SRPR) gelişen bir olguyu paylaştık.
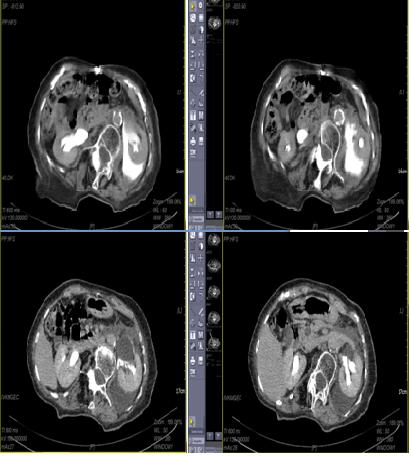
OLGU: 86 yaşında bir kadın hasta acil kliniğine son 7 gündür devam eden sol yan ağrısı ile başvurdu. Hastanın bir ay önce tanı almış sol böbrek taşı olduğu ve tedavi olarak hidrasyon ve analjezik aldığı öğrenildi. Ağrı son 24 saatte artmış ve hastada bulantı, kusma ve karnın sol tarafında hassasiyet gelişmiş. Yapılan USG’de sol hidronefroz ve sol perinefrik alanda abondan sıvı koleksiyonu görüldü, sağ böbrek normaldi. Sonrasında İV kontrastlı abdominopelvik tomografi çekildi; UPB’de 8 mm taş, sol perinefrik sıvı koleksiyonu, kontrast ekstravazasyonu görüldü ve sol renal pelvis rüptürü tanısı kondu (Şekil 1). Tetkiklerinde lökosit düzeyi 14.900, üre ve kreatinin normaldi. Ağrı kontrolünün ardından hastaya floroskopi altında sol DJ tatbiki uygulandı. Operasyonun ardından hastanın genel durumu birkaç saat içinde daramatik olarak düzeldi. Postoperatif 3.günde hastaya kontrol tomografi çekildi. Perinefrik alan öncekinden daha temiz izlendi ve sıvı koleksiyon azalmıştı. Taburculuk sonrası postoperatif birinci ayda hastaya bir seans SWL uygulandı, hasta taşsız hale geldi. SWL sonrası 2. haftada DJ stent çekildi.
Sonuç: SRPR çok nadir görülen bir durumdur. Bilinen en yaygın sebepleri ürolitiyazis, tümör, striktür, renal kistler, retroperitoneal fibrozs, hamilelik ve vezikoüreteral reflüdür. SRPR semptomları renal kolikle benzerdir. USG ve İVP tanısında ve ayırıcı tanısında kullanılır. Tanıda en değerli görüntüleme yöntemi İV kontrastlı tomografidir. Tedavisi altta yatan patolojiye yöneliktir. DJ stent veya perkütan nefrostomi üriner diversiyon amaçlı özellikle küçük boyutlu rüptürlerde kullanılır. Açık cerrahi onarım büyük boyutlu rüptürlerde bir seçenek olarak kullanılabilse de laparoskopide tedavi alternatiflerinden biridir. Gözlem veya medikal tedavi ile konservatif düşürülmesi beklenen taşlarının renal pelvis rüptürüne yol açabileceği akıllarda tutulmalıdır. Hastanın kliniğindeki ani bozulmalarda ayırıcı tanıda renal pelvis rüptürü de olmalıdır.
A complication of urolithiasis, spontaneous renal pelvis rupture
Arif Özkan, Nusret Can Çilesiz, Fatih Yanaral, Buğra Çetin, Memduh Aydın, Barış NuhoğluOBJECTIVES: Some ureteropelvic junction (UPJ) stones are mediated by observation and medical expulsive treatment. Some are complicated with urinary tract infection, hydronephrosis, and renal function disturbances. So surgery should be performed. Spontaneous perforation of UPJ is a rarely condition that poses diagnostic and therapeutic problems. We reported a case with a spontaneous renal pelvis rupture (SRPR).
CASE: An eighty-six year old woman has been admitted to emergency department with flank pain for last seven days. She had a UPJ stone for a month and hydration and daily oral analgesic were recommended to the patient. The pain increased in the last 24 hours, and patient has nausea, vomiting and tenderness in the left abdomen. Left hydronephrosis and abundant fluid collection in perinephric area were seen in ultrasonography. Then computerized tomography was performed and rupture of renal pelvis, perinephric fluid accumulation, contrast extravasation, and a 8 mm stone in UPJ were seen. Leukocyte level was 14900. Creatinine and urea were normal. After pain control, D-J stent was inserted under-fluoroscopy. After the operation patient’s clinical status was dramatically improved in a few hours. In control CT at postoperative third day, the perinephric area was clear and fluid collection was decreased. One session SWL was performed at postoperative 1st month. After the SWL patient become stone free. D-J stent was taken out after 2 weeks.
RESULTS: SRPR is an extremely rare condition. The most common abnormalities that have been reported are lithiasis, tumors, stricture, renal cysts, retroperitoneal fibrosis, pregnancy and vesicoureteral reflux. SRPR has the same symptoms as renal colic. Ultrasound and intravenous pyelogram are used in diagnosis and differential diagnosis. Intravenous contrast tomography is the most useful diagnostic tool. Treatment is according to underlying pathology. D-J stent or percutaneous nephrostomy is urinary diversion method to be used especially in small ruptures. Open surgery or laparoscopy can be an option with large rupture of renal pelvis. In ureteral stones expected to pass under observation or treated with medical expulsive treatment, the possibility of renal pelvis rupture should be kept in mind. In sudden clinical deterioration, it can be the first thing to come to mind.
Şekil 1: BT görüntüsü
Figure 1: CT image
)